Enteral Feeding and Colostomy Care Continuing Education Courses in New England
Enteral nutrition is the provision of nutritional support directly through the gastrointestinal tract. Patients eligible to receive longer term enteral nutrition, as often seen in the community, would have a functioning and accessible gastrointestinal tract, including those with swallowing disorders, such as motor neurone disease and multiple sclerosis; those with physical obstruction to swallowing, such as oesophageal tumours; those unable to ingest food, such as those with head injury or stroke; and those with anorexia due to an underlying disease, such as chronic lung disease, irritable bowel disease or cancer. Patients with dysphagia, anorexia, malabsorption or excessive catabolism may also need long-term enteral feeding (Pearce and Duncan, 2002).
An enteral feeding tube could be placed via a jejunostomy (percutaneous endoscopic jejunostomy (PEJ)) or a gastrostomy, (percutaneous endoscopic gastrostomy (PEG)), with the latter being more common (National Institute for Health and Care Excellence (NICE), 2017). Good nursing care practice would involve awareness of infection control and cleaning of these areas. The site of entry would need to be wiped clean and kept dry so as to prevent any environment being conducive to bacteria growing and an infection starting. An infection at the site of the wound could gain entry systemically and cause sepsis. The tube should be replaced as often as required in accordance with the provider's instructions.
Enteral feeding is now commonplace in the community due to the wide variety of resources and community staff that are able to manage long-term conditions such as those requiring this type of nutritional support being available in the patient's home. There has been an emphasis in recent years in managing long-term conditions increasingly in the community and reserving the more acute care issues for the hospitals, echoing the emphasis on community work set out in the NHS Long Term Plan (NHS England, 2019). Community nurses and other community healthcare practitioners should be aware of the NICE (2017) guidelines, which stipulate how to prepare and give enteral feeds, and discuss the use of the equipment involved, so as to prevent infection or unwanted problems that may lead to hospital admission, such as tube displacement or gastric perforation. Training is essential in the care of enteral feeding tubes (NICE, 2017). Community nurses have access to enteral feeding courses and courses relating to nutritional support. They can contact the nutrition support nurse for advice but also train within this speciality to manage patients with a PEG.
Percutaneous endoscopic gastrostomy
Percutaneous endoscopic gastrostomy (PEG) tubes are used for enteral feeding. These are long-term, artificial enteral feeding tubes suitable for adults and children that require endoscopic placement, allowing direct access to the stomach from outside the abdominal wall, and supplementation of nutrition, fluids and medication can be administered via these tubes (Haywood, 2012).
PEG tubes are usually made from flexible polyurethane and are approximately 35 cm in length, with a hollow lumen that allows for the passage of liquids (Haywood, 2012). On placement, the tube is held by a soft, malleable silicone- or air-filled foam sac retention bumper that lies against the anterior gastric wall. The bumper keeps the tube from coming out of the stomach (Cyrany et al, 2016).
The PEG tube is usually surgically inserted as a day case in the hospital by an appropriately qualified and specialist trained healthcare professional. The ideal would be for the tube not to move freely in the fistula tract but also for it not to fit too tightly (Haywood, 2012), preferably about 1 cm from the abdominal wall (Haywood, 2012).
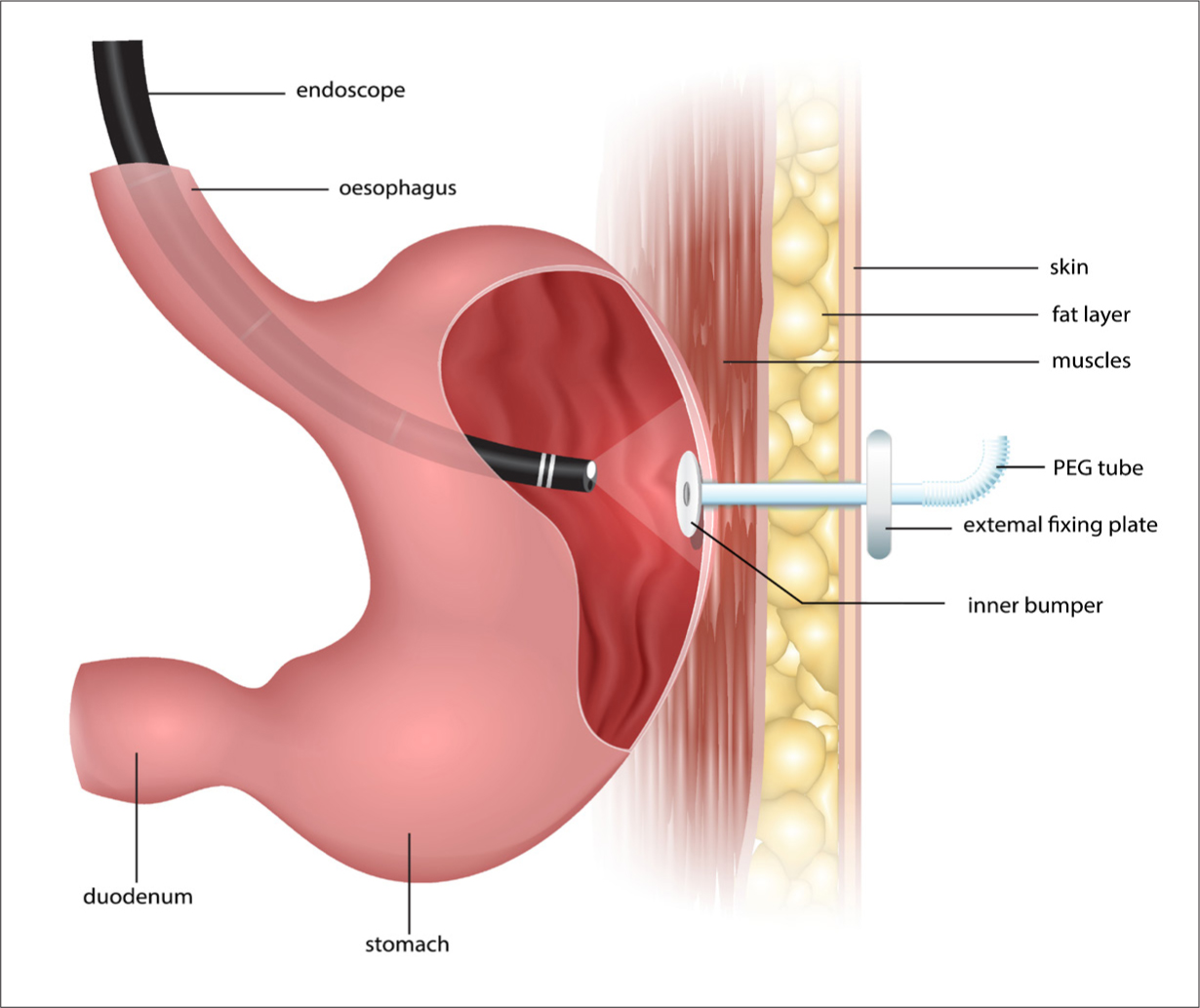 Figure 1. Placement of the percutaneous endoscopic gastrotomy tube for enteral feeding
Figure 1. Placement of the percutaneous endoscopic gastrotomy tube for enteral feeding
Any equipment used for giving feeds should be handled in an aseptic way so as to prevent contamination that could lead to infection or sepsis, and feed-giving sets should be discarded after each feeding session (NICE, 2017). The entrance site of the feeding tube should be washed daily with water and dried thoroughly (NICE, 2017). Care of the site of the wound would involve visits three times a week, usually, during which the wound site would be cleaned and checked for signs of infection, the tube would be checked to ensure it is in date and is not blocked and signs of any complications would be identified. The patient should be positioned upright for feeding and fully informed of what is happening throughout the visit.
Preparing and giving the feed
When preparing and giving feeds, cartons containing feeds that are ready to use and do not need mixing or diluting should be provided, which can be given in a feeding session of up to 24 hours (NICE, 2017).
To prevent blockages, the feeding tube should be flushed with freshly drawn up tap water before and after feeding or giving medications, using enteral syringes (NICE, 2017). For patients who are immunosuppressed, the water should be boiled and then cooled, or sterile water should be used from a freshly opened container, so as to further prevent the risk of infection (NICE, 2017).
In situations where ready-to-use feeds are not available, the person preparing the feed should wash their hands thoroughly and work in a clean working area with equipment that is only to be used for enteral feeding (NICE, 2017). Only cooled boiled water or fresh sterile water should be used when mixinf a feed, which can be prepared up to 24 hours in advance and kept in the fridge. Once mixed, the feeding session should last no more than 4 hours (NICE, 2017).
Red flag alerts
Complications of PEG insertions include bleeding, intestinal/colonic perforation, post-insertion trauma, discomfort, erosions, fistulae and strictures. Displacement can occur where the tube falls out, whereby the tube may cause bronchial administration of the feed leading to reflux oesophagitis or aspiration. Gastrointestinal intolerance can also occur, causing nausea, bloating, pain and diarrhoea. Metabolic refeeding syndrome can also be a complication, as well as hyperglycaemia, fluid overload and electrolyte disturbance.
The National Patient Safety Agency (NPSA) (2010) developed red flag alerts to be aware of in related to the period after enteral tube insertion. These include:
- Severe pain that is not relieved by simple analgesia, or is made worse by using the tube
- Fresh bleeding (a small amount of bleeding is expected; avoid large thick dressings that disguise heavier bleeding) or gastric fluid or feed leaking from the wound site
- Sudden change in clinical observations
- Change in patient's level of responsiveness or behaviour.
These symptoms are signs of complications, and urgent medical attention should be sought if any of them appear. With good nursing care, many of the associated complications can be avoided or highlighted promptly for investigation and management (Haywood, 2012).
Communication and the MDT
A healthcare professional looking after patients in the community should ensure that the patient and carer are kept fully informed of any change in care resulting from an identified complication. They should also be kept informed of when the tube needs replacing, and when to expect visits, additional appointments for review, specialist contact, etc. Further, access should be made available to appropriate sources of information in the correct format, language and ways appropriate to the individual's requirements. NICE (2017) stated that it is important to consider the patient's cognition, physical needs, stage of life and culture and that they should be given the opportunity to discuss their diagnosis, treatment options and all the relevant physical, psychological and social issues, encompassing more holistic care of the patient. It is important to provide contact details of places that may help provide support, such as the relevant support groups, charities and voluntary organisations.
NICE (2017) guidelines also stated that all people in the community setting who are receiving enteral feeding should have the support of a coordinated multidisciplinary team (MDT), including dietitians; district, care home or homecare company nurses; GPs; community pharmacists and other allied healthcare professionals (for example, speech and language therapists), as appropriate. There should be close communication between the MDT and patients and carers regarding the patient's diagnoses, prescription, arrangements and potential complications or problems. There should be a care plan tailored individualistically to the patient's needs, which would cover the overall aims and a monitoring plan.
Appropriate training for the patient and their carer is essential, with regard to the management of the tube, delivery system and regimen, and an outline of procedures that relate to setting up the feed, using the feed pump, the likely risks and methods for troubleshooting common problems, and there should also be provision of an instruction manual and if appropriate, visual aids (NICE, 2017).
Routine and emergency telephone numbers to contact a health professional who understands the needs and potential problems of people on home enteral tube feeding, the delivery of equipment, ancillaries and feed with appropriate contact details for any homecare company involved should also be provided to the community patient who is receiving enteral nutrition (NICE, 2017).
Conclusion
The main considerations for community practitioners caring for those requiring enteral feeding involve an excellent standard of cleanliness and technique when caring for the feeding tube and administering the feed, as well as the psychosocial considerations of the patient alongside their physical clinical care. The organisation required for when the patient has had their PEG inserted is significant, and continuing care surrounding nutritional support, with attention paid to holistic needs is also of great importance. Red flags and complications to look out for should be kept in mind, and basic aseptic principles should always be followed as best as possible in the community, with appropriately trained staff managing the PEG tube and the required nutritional input. Different feeds and their individual instructions with regard to mixing and use should also be considered. Keeping the patient and carer trained and informed in managing the nutritional intake and avoiding complications are essential throughout the care of these patients in the community setting.
KEY POINTS
- Percutaneous endoscopic gastrotomy (PEG) tubes are inserted surgically in the hospital as a day case and managed by a wider multidisciplinary team (MDT) in the community
- Patients and carers must be informed and trained, and factors such as patient cognition should be considered when attempting to manage potential for risks and complications
- Some patients require more support than others in managing their PEG; the MDT should consider this in a tailored care plan
- Red flags may be seen post insertion, in the community, such as fresh bleeding and severe pain. Careful attention must be paid in the early days following insertion and urgent medical attention sought where these complications are observed
- Holistic care of the psychological and physical health of the patient should be given
CPD REFLECTIVE QUESTIONS
- Reflecting on a patient from your caseload who had a percutaneous endoscopic gastrotomy (PEG) tube, describe how you safely managed the tube, delivered nutritional support and identified potential complications
- How you communicate with the wider multidisciplinary team about the patient's physical health while also looking after their mental health?
- What are the key ways to help manage the patient's wellbeing? Think of what would be included on an individualised care plan for the patient, bearing in mind a more holistic view of their overall health
Source: https://www.britishjournalofcommunitynursing.com/articles/an-overview-of-enteral-feeding-in-the-community/
{kind=link}
Post a Comment for "Enteral Feeding and Colostomy Care Continuing Education Courses in New England"